
The Measles Cure We've Ignored
Not sure why I did this, but here it is. Might be useful someday, somewhere to someone, maybe in the 3rd world, or in Texas.

With measles back in the news again due to the suspected outbreak in Texas some people who like to be prepared for any eventuality are concerned and asking about treating measles were it to become more widespread, or if it were to unaccountably become suddenly more pathogenic.
Many older readers, eg those in RFK Jr’s cohort, will remember getting measles and that generally speaking it was no big deal. Mainstream sources claim prior to vaccines became widespread there were something like 45,000 hospitalized per year and perhaps a few hundred deaths. Some got severe complications like pneumonia and brain inflammation, and it also wiped away immune memory, which could last months to years, leading to subsequent infections with other pathogens.
Now this post takes more of a functional medicine approach to the topic, rather than a deeply traditional one. From one perspective you could argue that what some label infections are simply the body’s regularly scheduled detox protocol - the rash, cough/mucus, sweating, diarrhea, vomiting, etc of various acute infectious diseases are all means to expel toxins that have accumulated over time and get rid of old, weak cells, replacing them with brand new, more vital ones.
From this point of view, a strong immune system is one which will make you sick as and when needed, and a weak one may not make you acutely ill much at all. Within this paradigm it’s possible that those at risk of complications wouldn’t sustain quite so many of them if there were no well-intended medical intervention made to assist them, since medical interventions so often get in the way of the body doing what it needs to do to keep you alive, frequently by covering up necessary symptoms, which are really just evidence of the immune system doing its job.
Or maybe some people really are at risk, maybe they really are too weak to put up with the infection their body takes on, and without intervention perhaps they will develop severe complications or even die (I don’t know, I might bet on the first view myself, but wouldn’t blame anyone for betting on the second).
From this perspective we’re left trying to manage infections with often dangerous and poorly considered mainstream approaches, like those featured during the COVID-19 pandemic, or putting on our thinking caps and creating our own protocols based on knowledge of disease pathogenesis and a review of the literature, much like various groups did to great success during the COVID-19 pandemic.
And that’s what we’re trying to do here. Create a functional medicine protocol that might be generalizable across many different patient populations and countries.
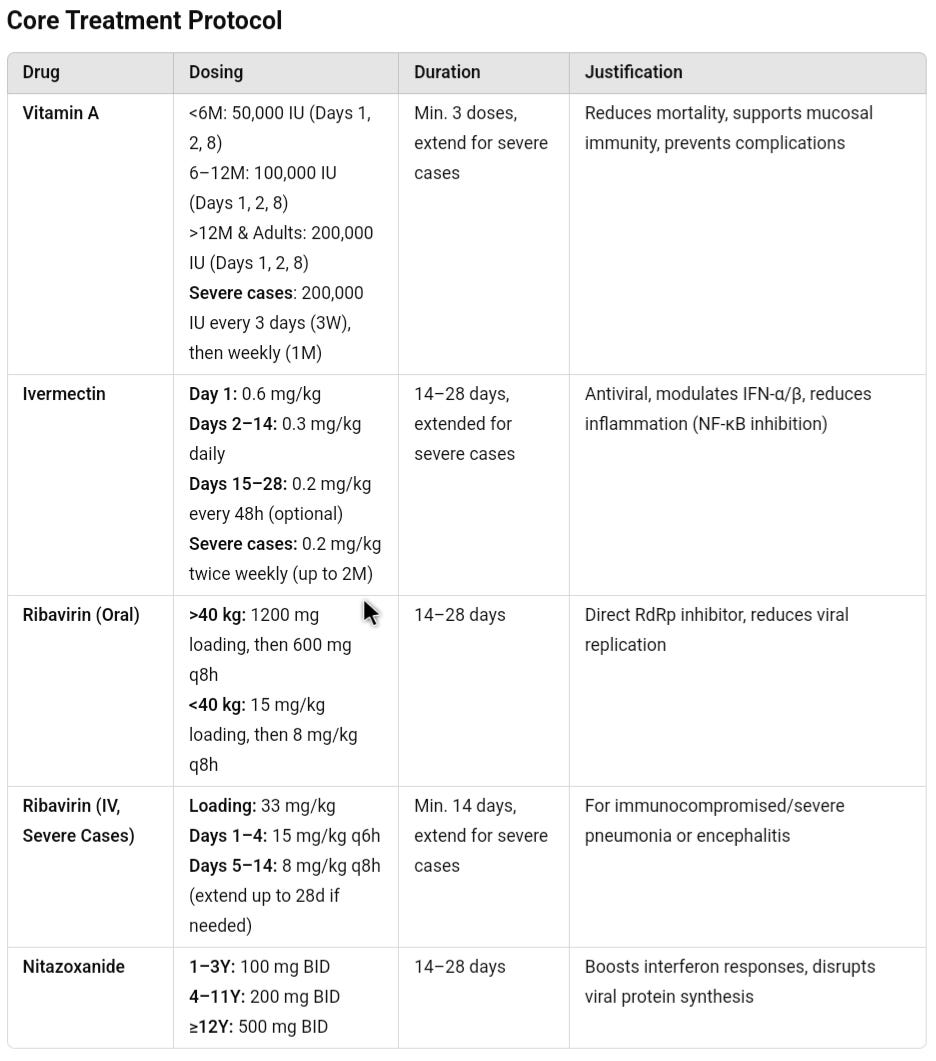
So we’ll cover the most important vitamin for measles prevention and treatment, along with the common off label meds that studies have shown have antiviral and anti-inflammatory effects that may be helpful to treat measles. We'll also theorize about prescription and over the counter medications, supplements and herbs that could be added based on measles’ pathogenesis, going into their mechanisms of action and dosing. Finally we’ll wrap up with a thorough review of the many important lifestyle measures and their mechanisms in supporting healing.
To avoid burying the lede, I’ll just say here that it is entirely possible, though based on sparse clinical research, that we already know how to cure measles in most cases: a combination of high dose vitamin A and ribavirin. The vitamin A alone reduces mortality 70% in high risk populations without good access to supportive ICU care, and at least in 1 small trial of 100 patients ribavirin reduced mortality 100%.
I was surprised to find the evidence suggesting these were likely to be very effective, yet despite ribavirin being a definitive measles antiviral it isn’t much used, probably because there is a significant risk of side effects including many uncomfortable ones like muscle, joint and stomach pain, nausea, depression, anxiety, and many clinically dangerous ones like a 10% incidence of hemolytic anemia (in the trials where it was used that wasn’t generally a significant risk though, especially in closely monitored patients who could be transfused if necessary), but even more concerning a significant effect on child height growth curves with up to 12% chance of a drop of 30 percentile points that would be measured in the multiple inches if it persisted, with much higher chances of less severe but detectable height drops, so this alone would drastically limit the acceptability of ribavirin in all children, except the highest risk.
However, we can simply replace ribavirin with ivermectin, which has nearly identical mechanisms of action against measles and has essentially no significant side effects at any reasonable dose or duration that we have detected with extensive use before, during and after the COVID-19 pandemic.
Going beyond that we can actually create a much more robust protocol for measles in the same way that COVID-19 protocols were developed: addressing various pathologic features of infection, enhancing some suppressed areas of the immune response and calming certain overactive immune responses that may lead to self harm.
In the absence of any large confirmatory studies, the other key to successful treatment, just as in COVID-19 is likely to be early and aggressive multi-drug therapy (maybe some of the therapeutics expected to work based on theory don’t really work in the real world, so we spread our bets), and especially continuing that therapy for an adequate period of time - measles virus replication peaks around day 5 when the rash appears, but it can continue for up to 4 weeks after the first symptom. Continuing treatments past symptom resolution is likely to be important in ensuring recovery and preventing complications including “long measles” syndromes of immune dysfunction.
Measles, an RNA virus like COVID-19 has very similar pathogenetic features as COVID-19. Of course it hits different tissues harder, eg the rash is a much more prominent issue with measles, but the underlying causes of disease in the skin are similar to the underlying causes of disease in the lungs for COVID-19. The biggest clinical difference is that measles, unlike COVID targets immune cells and frequently leads to significant immune amnesia and exhaustion. However if we treat it with effective therapies that should be prevented.
Long story short you could probably simply use the same COVID-19 protocol built around ivermectin to treat measles, since ivermectin does everything ribavirin does, without the side effects, with one key difference: the day 8 steroid use that prevents severe disease, complications and long COVID should probably be shifted a couple days earlier since measles viral load peaks 2 days earlier than COVID-19 on average and therefore the immune over-activation would be expected to start 2 days sooner.
This turned into a relatively long post, and since not everyone is interested in all the exhaustive details that go into designing a measles protocol, I’ll just drop the summary points that most people are interested in here at the top (note: ribavirin reserved for patients who can be closely monitored for anemia and other severe side effects):

After expanding on the rational for the above, which makes up a good portion of the post, we’ll get into the possible herbal, nutritional and broader lifestyle approaches to treating measles successfully towards the end.
The Details
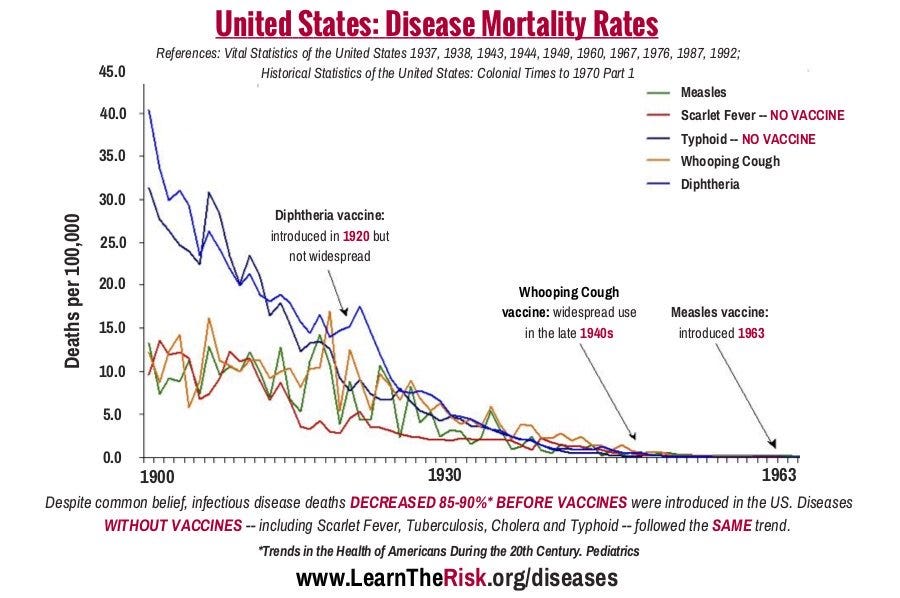
To set the stage it’s important to note that public data irrefutably shows that the incidence of viral diseases as well as their severity dropped anywhere from 90-99% before the introduction of vaccines during a historical period when the population measured was becoming better nourished, less crowded and more sanitary. The trend was always down for a variety of reasons, but vaccines swooped in at the end and took all the credit.
For example here is the historical data on the incidence of various common infectious diseases including Measles showing when their respective vaccines were introduced:
The impact of living conditions including general nutrition, micronutrient sufficiency, overcrowding, and sanitation to the risk of catching measles and being severely affected by it are not even the subject of mainstream scientific dispute.
But what is underappreciated by those living in the first world who already have generally good general nutrition and live in mostly uncrowded, sanitary conditions, is just how important vitamin A deficiency can be. Despite generally sufficient or even excessive caloric intake in the West, many suffer from important deficiencies of crucial micronutrients due to over reliance on processed foods, and sometimes artificial dietary restrictions that aren’t properly counterbalanced, e.g. veganism when it relies on plant sources of the beta carotene precursor to vitamin A, which isn’t present in it’s active form in plants (not everyone can convert beta carotene in sufficient quantities to create enough vitamin A, and the problem is worsened when the diet is deficient in bioavailable beta carotene to begin with due to an over concentration of processed foods).
Vitamin A Deficiency and Measles
The relationship between vitamin A deficiency and the risk of complications from measles is supported by substantial evidence, with multiple studies and clinical observations suggesting that vitamin A deficiency can increase the severity and risk of adverse outcomes in measles infections.
Theory & Mechanism of Action:
Vitamin A is crucial for maintaining the integrity of surface epithelial cells (e.g., skin and mucous membranes) that form the first barrier to infections, and for overall proper immune system function. For example it helps in the production of antibodies and in the function of T-cells, which are heavily involved in the body's immune response to infections like measles.
Since measles primarily affects the respiratory and gastrointestinal systems which are lined by mucosal cells, vitamin A's role in maintaining mucosal immunity is critical. Deficiency in vitamin A weakens these defenses, increasing susceptibility to both the virus itself and secondary bacterial infections which can lead to severe complications.
Supportive Observational Data:
As expected several studies have demonstrated that children who are vitamin A-deficient experience more severe complications from measles, such as pneumonia, diarrhea, encephalitis (brain inflammation that can cause seizures, coma, brain damage) and even death. In areas with high rates of malnutrition and low vitamin A intake, the risk of severe measles outcomes is significantly higher.
Supportive Prospective Interventional Studies:
Numerous clinical trials and interventions have shown that providing vitamin A supplements to children diagnosed with measles can reduce the severity of the disease and decrease mortality. For example, large-scale studies in Africa and Asia have shown that vitamin A supplementation alone (e.g. without addressing sanitation, overcrowding and protein calorie malnutrition) can reduce measles-related mortality by 50-70%.
Global health guidelines: Based on this evidence, the World Health Organization (WHO) and UNICEF recommend high dose vitamin A supplementation for 2 days for all children with measles (200,000 IU per day for 2 days, or 100,000 IU for infants), particularly in regions with high rates of deficiency. This recommendation is based on evidence that vitamin A supplementation not only reduces mortality but also shortens the duration and severity of the disease.
Importantly the recommendation is for retinol, the active form of Vitamin A found primarily in animal liver, and not for the plant based precursor beta carotene.
Applicability to Western Populations
While it’s true that evidence of benefit is more robust in underprivileged groups, given the low risk of 2 days of high dose vitamin A, this should be part of any protocol to treat or prevent Measles.
Signs that someone may be deficiency in vitamin A to begin with include a history of night blindness, dry eyes, pneumonia, severe or frequent infectious diarrhea and infertility.
Medications
Measles is an RNA virus, and many scientists believe ivermectin may be a broad spectrum RNA antiviral due to its mechanisms of action. There are also small isolated studies suggesting ribavirin and nitazoxanide (also used for COVID) have significant efficacy as measles antivirals (ribavirin showing 100% reduction in mortality), so in a high risk patients, or severe case it might be prudent to treat not only with high dose vitamin A, but all three of these antiviral, immune-modulating medications, with ribavirin reserved for those that can be monitored since it causes significant and possibly dangerous anemia in a relatively large percentage of patients.
Paywall note: as usual if you can’t afford to pay a small fee to support the publication you can email us at welcome@mygotodoc.com for free access to the below paid content section which goes into the details of the rest of the protocol including the rationale for the prescription and over the counter drugs and supplements, gives details on herbal approaches, nutritional support that could replace synthetic vitamins (yes, you can get 200,000 IU per day of vitamin A from reasonable quantities of food), and many additional lifestyle measures that are of the utmost importance for safely getting through measles or any other acute viral illness.
